Cholesterol is a measurement, not a verdict - Dr Vlad Gubala
A single cholesterol result is useful, but it is not a clinical truth handed down from above. It is one measurement in time, taken in a biological system that is constantly moving, and interpreted through an analytical method that has its own uncertainty [1,2,3].
That matters because lipids are not static. Classic data from the National Cholesterol Education Program showed day-to-day biological variation of around 5% for total cholesterol, 10% for HDL cholesterol and 20% for triglycerides, even before analytical variation is considered. In other words, your lipids are not a granite monument; they are more like a weather report. The weather, as we all know, is rarely impressed by our desire for certainty [3].
Analytical variation adds another layer. Between laboratories, platforms, calibrations and pre-analytical handling, the same sample can produce materially different answers, and published work has shown that these differences can be clinically meaningful. That is why a lipid result should always be read as an estimate with context, not as a definitive label. If this were mathematics, the answer would come with a confidence interval; biology is not obliged to be tidy [4, 5].
For cardiovascular disease risk, this distinction matters. Cholesterol is one risk factor, but not the whole risk picture. QRISK3 uses multiple variables, including the total cholesterol to HDL ratio, rather than relying on a single threshold crossing. That is a more sensible way to manage the noise inherent in biology. It also avoids the absurdity of making one test carry the entire weight of a clinical decision. Lipids are important - just not magical [6, 7].
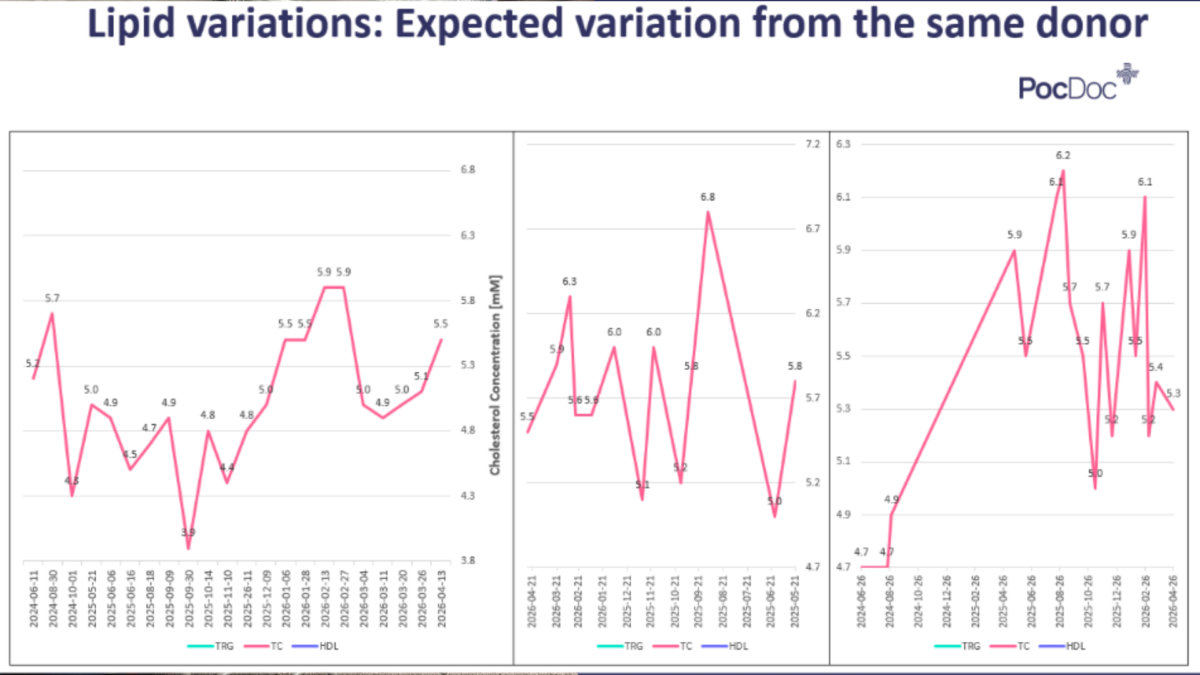
Real-world tracking data from three individuals tested repeatedly over 18 months confirms this: total cholesterol swings of 1.5–1.8 mmol/L within the same person, without any change in medication or major lifestyle intervention. The clinical implication? A lipid result is an input, not an output.
The practical message is simple. A rising or falling cholesterol value may reflect true change, but it may also reflect normal biological fluctuation, analytical variation, or both. Repeated testing, trend interpretation and risk-based assessment are therefore more informative than treating one number as a final judgement. In clinical chemistry, certainty is often overrated; consistency and context usually win [8].
For me, the key takeaway is this: lipid testing is not about worshipping a number, it is about understanding risk. The result is a snapshot, not a verdict. And if the snapshot looks slightly different next time, that does not necessarily mean the patient has changed - sometimes the measurement simply moved first.
Get in touch to find out more




